
WHAT WAS THE PROBLEM?
The Kingdom of Eswatini has the highest HIV prevalence in the world, yet fewer than half of HIV-exposed infants are retained in care long enough to receive their final HIV status at 18–24 months. Mothers and infants receive care together at child welfare visits through 18-24 months postpartum/of age, but there are high rates of loss to follow-up (LTFU) of mother-baby pairs (MBP) after the six-week visit. This poor retention in care limits the impact of prevention of mother-to-child HIV transmission (PMTCT) services as well as linkage to antiretroviral treatment (ART) for HIV-positive infants and HIV care and treatment services for HIV-positive mothers. LTFU of MBP also prevents them from receiving critical maternal, newborn, and child health (MNCH) services, including immunizations, growth monitoring, and supplements for infants – and family planning, infant feeding counseling, and cervical cancer screening for mothers.
WHAT IS THE SOLUTION?
CFMs are trained to provide proactive community-level follow-up of all MBPs at their homes to encourage them to attend all child welfare visits at the health facility. Health facilities enroll all MBP, regardless of HIV status, at the six-week postpartum visit and assign them to a CFM for follow-up in the community. CFMs visit mothers with new babies at their homes to create a plan to help them attend all child welfare visits in the following 18-24 months and to discuss challenges that might prevent them from completing all visits. Each month, CFMs update this care plan with anticipated changes in the MBP’s location or the child’s caregiver, problem-solve barriers to completing visits, provide referrals to MBPs who have missed a visit, and ensure that the baby’s Child Health Card is up-to-date. Rather than waiting to conduct defaulter tracing after missed appointments, this proactive model has CFMs work with MBP before any are lost to follow-up and provide support to prevent missed visits.
The Kingdom of Eswatini MOH has made efforts to integrate all MBP care to improve access and uptake of necessary health services (including HIV testing and ART services) by aligning them with child welfare visits. By encouraging clinic attendance together for monthly visits and helping mothers plan for the next visit, CFMs ensure that both mothers and infants receive HIV testing services per the MOH protocol. By having CFMs visit all homes in the community with new babies, not just those with HIV-exposed infants, this model also reduces concerns of HIV stigma and accidental disclosure – key barriers to HIV care in Eswatini. In addition to HIV services, this retention in care model also helps MBP receive critical MNCH services, including immunizations and growth monitoring for infants, and family planning counseling, infant feeding counseling, and cervical cancer screenings for mothers. While designed to improve PMTCT final outcome rates, by ensuring retention in care, CFMs help improve uptake of other crucial MNCH services. This integrated PMTCT and MNCH outreach can improve outcomes for HIV testing and early infant diagnosis, as well as address gaps in follow-up of mothers and infants during the critical period of 18-24 months.
WHAT WAS THE IMPACT?
Comparison to baseline data reveals the success of the CFM model in improving retention in care. Baseline data collected in 2017 at the three intervention clinics showed that retention in care in the 2015 cohort of infants dropped sharply after the six-week visit to 70 percent / 64 percent of infants (HIV-exposed / unexposed) at the six-month visit and 46 percent / 39 percent at 12 months (Figure 1). AIDSFree has seen 100 percent retention in care of HIV-exposed and unexposed infants enrolled in the program to date for all age-appropriate visits per the MOH schedule (Table 1).
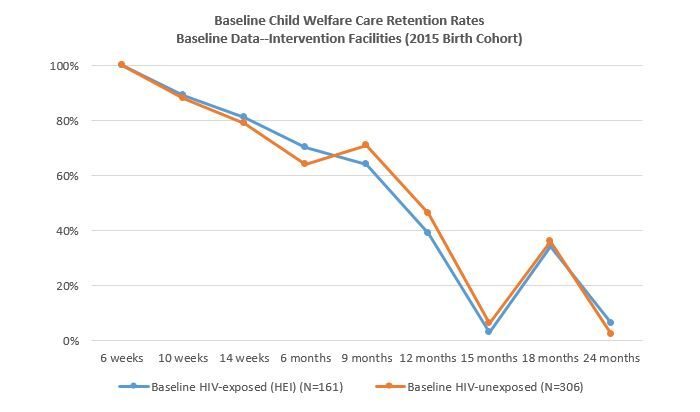 Figure 1. Low retention rates at child welfare clinics after six weeks of age prior to intervention (2015 Birth Cohort)
Figure 1. Low retention rates at child welfare clinics after six weeks of age prior to intervention (2015 Birth Cohort)
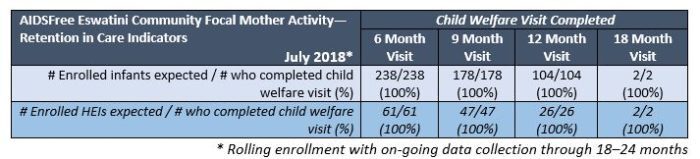
Table 1. Retention Rates at AIDSFree Community Focal Mothers Facilities (July 2018 – Rolling enrollment)
HOW DOES IT WORK?
INDIVIDUAL LEVEL
Mother-Baby Pair Enrollment: Mothers with new babies are made aware of the program when they visit the health facility for their six-week postpartum visit. A nurse or health facility staff member discusses the benefits of the program with them, provides them with information in siSwati (local language), and talks through any questions or concerns. Mothers who agree to home visits complete an enrollment form with their contact information. CFMs use that information to contact the mother to arrange the initial home visit.
Home Visits: CFMs conduct monthly home visits with new MBP, with follow-up visits as needed. During these visits, they encourage the mothers to attend child welfare care per the MOH schedule. At each home visit, CFMs review the MOH Child Health Card and develop a care plan with the mother to prepare for clinic visits and anticipate potential changes in location of the mother and/or baby, or changes in the baby’s caregiver, which are reviewed at each subsequent home visit.
Role of CFM: CFMs are trained on HIV and PMTCT basics, communication skills, confidentiality, the MOH child welfare care service package, and reading the MOH Child Health Card. While some may have previous volunteer experience, CFM training stresses the importance of adherence to clinic visits for the baby’s and mother’s health. Their emphasis is on encouraging clinic visit attendance and preventing defaulters. Their role is focused to allow them to concentrate on problem solving and proactive planning and follow-up with MBP. Each CFM follows 15-20 MBP. CFMs complete a home visit with each mother-baby pair every month, usually visiting one to three MBPs per day, but the schedule of the home visits and visits per day varies based on geographical factors and mother-baby pair availability.
Support for CFM: AIDSFree serves as the CFMs’ primary supervisor. CFMs meet twice per month at the clinic with AIDSFree supervisors and health facility focal persons to receive assignments of new MBP, discuss home visits, review tools/data collected, request additional support, and troubleshoot any challenges encountered during home visits. CFMs receive a monetary stipend in an amount determined by similar lay worker stipends in Eswatini. Additionally, CFMs are provided with airtime vouchers to support follow-up calls to mothers, as well as a support package which includes a t-shirt, name badge, a tote bag, and a sun hat.
SERVICE DELIVERY LEVEL
Improvements in Service Delivery: Eswatini has integrated MNCH care at the child welfare visit in order to streamline service delivery and improve service uptake. For infants, child welfare care encompasses monthly growth monitoring, immunizations, vitamin A supplementation, deworming, and early childhood development services. Mothers also receive critical health services at these child welfare visits, including family planning counseling, infant feeding counseling, and cervical cancer screening. Retention in this care is critical, as improving this also increases the uptake of these key health services during the postpartum/postnatal period. A data review of infants enrolled in home visits demonstrates that they have all been retained in child welfare care and have received all key health services per the MOH schedule.
All infants who present at the six-week visit are enrolled, regardless of HIV status. Lactating mothers receive HIV testing at all child welfare visits per the MOH schedule, as incident HIV infection during pregnancy and breastfeeding contributes to a significant proportion of infants with HIV in high incidence settings.[1] While to date, two infants have tested HIV-positive, no incident maternal HIV infections have been identified in the enrolled mothers. By encouraging clinic attendance together for monthly visits for all MBP, this model supports both mothers and infants to receive HIV testing services per the protocol for PMTCT, leading to better outcomes. It also avoids HIV stigma and accidental disclosure in the community by having CFMs visit all homes with new babies, not just those with HIV-exposed infants.
Given the success of the CFM in proactively retaining MBP, and linking those who miss visits back to care – which also ensures that mothers are receiving key services including ART and VL testing per the MOH schedule – the Sexual and Reproductive Health Unit (SRHU) is initiating plans to train Global Fund-funded mentor mothers using the AIDSFree CFM model and training materials in late 2018. The role will be expanded with an enhanced focus on maternal ART adherence support, including follow-up of mothers who default from ART care or seek ART services in facilities separate from their child welfare care. This enhanced role has the potential to improve maternal ART adherence and VL, thereby helping to reduce vertical transmission.
HEALTH SYSTEMS LEVEL
The CFM model strengthens health facilities’ access to community-level information about MBP’s location and mobility, which can improve facility data quality. MBP that were previously recorded as lost to follow-up can be identified by CFMs as transfers-out to other health facilities, which can then be confirmed by the receiving facility.
This intervention also offers an opportunity for health facility staff to identify data quality issues in the health facility register. At home visits, CFMs record information from the Child Health Cards and are able to ensure it matches what was recorded in the health facility register. This helps facility staff to identify when information has been left out of the register and correct register data quality issues early.
NATIONAL ENVIRONMENT
AIDSFree has implemented this intervention in close collaboration with the MOH, with regular reporting to the Sexual and Reproductive Health Unit and the PMTCT Technical Working Group. Eswatini is focused on improving its rates of PMTCT final outcome and has supported this program with strong buy-in. One challenge, however, is that MBP are currently not yet linked in MOH facility registers – linking mothers and their infants in multiple registers continues to impact data collection and reporting. Future national efforts to link MBP are anticipated.
AIDSFree has also successfully engaged regional or facility social workers in the event that a CFM identifies an issue of concern in a home that she visits. Linkage with the social workers have been very effective in allowing them to work with the concerned parties and address the situation using the guidelines stipulated by the Deputy Prime Minister of the Kingdom of Eswatini.
SCALABILITY
The model is focused on MBP retention in care to allow CFM to concentrate on problem solving and proactive follow-up at the community level before a mother misses a visit. This approach allows CFMs to direct their efforts towards targeted monthly home visits with a larger cohort of MBP. By keeping CFMs focused, this model allows for the rapid scale-up in communities. Keeping the ratio of 15-20 MBP per one CFM is recommended as is regular evaluation of CFM workload by the supervising team.
At the request of the MOH, AIDSFree is currently working closely with the SRHU to plan national rollout the CFM model to increase the number of infants who know their final HIV status at 18-24 months and improve the rate of PMTCT final outcome determination throughout the Kingdom of Eswatini. Under the leadership of the SRHU, AIDSFree has developed a full training package, standard operating procedures (SOPs), and job aids. The MOH will be able to roll out the program nationally via a cadre of “mentor mothers” that are being hired with funding from the Global Fund. The role is anticipated to provide proactive follow-up of MBP and expand to also focus on maternal ART adherence support for those who default in care or seek ART services at separate facilities from their child welfare care. This model could also be integrated into larger training packages, including potentially exploring the initiation of proactive follow-up during the postpartum period with continuous MBP follow-up through 18-24 months. In other contexts, enrollment could be considered at the seven-day visit, or at delivery, if retention at the six-week visit is low.
BUDGET
Start-up Costs: Start-up costs include an initial landscape analysis for identification and outreach to community leaders as well as the identification and training of CFMs. This process also helps ensure full community buy-in and to also determine if there are existing community cadres that may be well-placed to absorb the CFM role without loss of program effectiveness.
A key variable is determining how many CFMs should be trained and assigned to each Chiefdom and health facility. The number of CFMs will vary by several factors, including: the number of MBP enrolling per health facility; geographic considerations in each Chiefdom; and maintaining the ideal ratio of CFMs to MBP (1 to 15-20). To determine the number of MBP likely to enroll per health facility, AIDSFree estimated expected birth cohort size by facility with previous year birth cohorts. When determining the number of CFMs required for each Chiefdom (or region/district in other settings), it is essential to consider CFMs’ workload ability. Once the number of CFMs is identified, candidates are recruited and trained by the program coordinators and supervisors. The scale of the training will vary by the size of the program.
Cost Drivers: The cost drivers for the implementation of the CFM model include: (1) training of CFMs, (2) ongoing supportive supervision – which includes biweekly group meetings at the implementing health facilities, particularly important to ensuring strong bi-directional communication with facilities; (3) a monthly stipend for CFMs as well as a support package (t-shirt, tote bag, sun hat); and (4) the printing of materials, including the community register, care plans, and home visit checklists.
To learn more about AIDSFree’s mother-baby pair retention activities, click here.
*This blog was originally published by PEPFARSolutions.


