
Currently, 1.7 million children around the world are living with HIV, and they often face distinct challenges in adhering to treatment. As a result, EGPAF has spearheaded efforts to provide individualized care and attention to address these unique needs and barriers.
In 2007, EGPAF created the Ariel Club model. Named after the daughter of Elizabeth Glaser, Ariel, who lost her own battle with AIDS in 1988, this model became a replicable and customizable approach to address the needs of children and youth across several contexts and age groups. There are now 500 Ariel Clubs active across nine EGPAF-supported countries: Côte d’Ivoire, Democratic Republic of the Congo, Eswatini (formerly Swaziland), Kenya, Lesotho, Malawi, Mozambique, Tanzania, and Uganda.
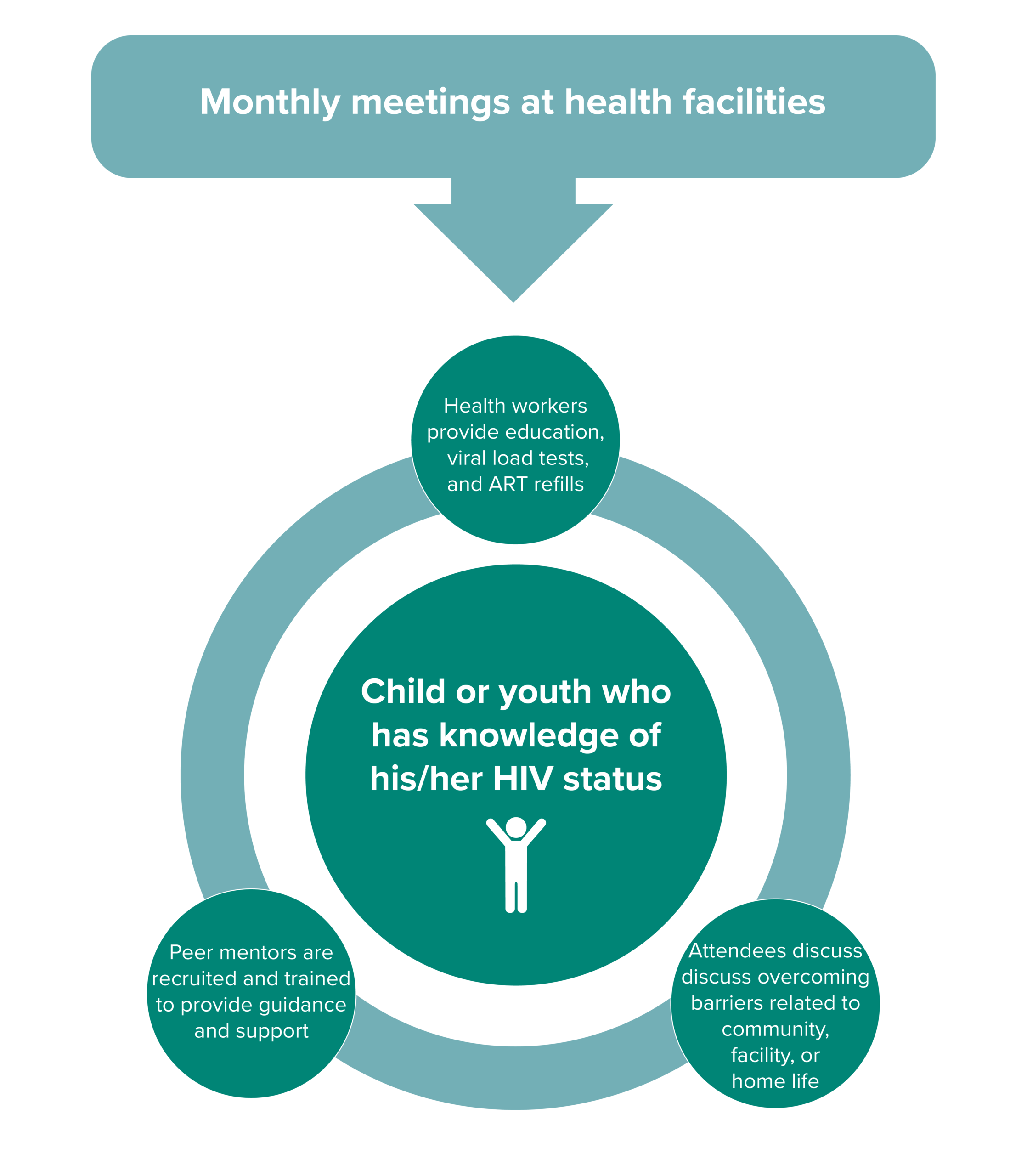
The clubs are specialized in each country to ensure they address local challenges and the realities of young patients in care. However, key service delivery includes regular check-ins at clinics, viral load testing and antiretroviral therapy (ART) refills managed on site, and health education. These regular check-ins allow children and youth to engage with peers to dispel stigma. Attendees feel they are not alone in this process of disclosure, acceptance of lifelong treatment, and (oftentimes) enduring discriminatory behaviors in their own communities. The clubs offer help, understanding, and support led by peers and health workers.
Several countries have taken this base model and added other important components to the individuals they aim to serve. Some have created age-specific or sex-specific groups, and some have invited caregivers in for special sessions on how they can support their HIV-positive child or adolescent in the treatment paradigm.
Read the Ariel Clubs Case Study and learn more in the PEPFAR Solutions Database Profile: Ariel Adherence Clubs in Tanzania.
Ariel Adherence Club Benefits for Children & Youth Living with HIV
-
Improved retention on ART, adherence, and viral suppression among participants
-
Increased capacity of service providers to effectively communicate with, and provide quality HIV services to, children and adolescents
-
Provided support and guidance for caregivers of children and adolescents living with HIV, particularly for disclosure and retention in care.
-
Psychological support for children and adolescents living with HIV
-
Age-appropriate discussion and information sharing on healthy living and nutrition
-
Gender- and age-sensitive information and discussion on sexuality and sexual health, including reducing the risk of HIV transmission to sexual partners and undetected = untransmittable (U=U) messaging.
-
Development of peer educators to improve HIV support among adolescents preparing to transition to adult care
-
Provision of a safe, fun, and socially engaging space for children and adolescents living with HIV
-
Medication dispensing to decongest facilities